Case Studies in Telehealth Adoption
January 2013
![]()
The mission of The Commonwealth Fund is to promote a high performance health care system. The Fund carries out this mandate by supporting independent research on health care issues and making grants to improve health care practice and policy. Support for this research was provided by
The Commonwealth Fund. The views presented here are those of the author and not necessarily those of The Commonwealth Fund or its directors, officers, or staff.
The Veterans Health Administration: Taking Home Telehealth Services to Scale Nationally
An d r e w Br o d e r i c k
ABSTRACT: Since the 1990s, the Veterans Health Administration (VHA) has used infor- mation and communications technologies to provide high-quality, coordinated, and com- prehensive primary and specialist care services to its veteran population. Within the VHA, the Office of Telehealth Services offers veterans a program called Care Coordination/ Home Telehealth (CCHT) to provide routine noninstitutional care and targeted care man- agement and case management services to veterans with diabetes, congestive heart fail- ure, hypertension, post-traumatic stress disorder, and other conditions. The program uses remote monitoring devices in veterans’ homes to communicate health status and to cap- ture and transmit biometric data that are monitored remotely by care coordinators. CCHT has shown promising results: fewer bed days of care, reduced hospital admissions, and high rates of patient satisfaction. This issue brief highlights factors critical to the VHA’s success—like the organization’s leadership, culture, and existing information technology infrastructure—as well as opportunities and challenges.
For more information about this study, please contact:
Andrew Broderick, M.A., M.B.A. Codirector, Center for Innovation
OVERVIEW
and Technology in Public Health Public Health Institute abroderick@phi.org
To learn more about new publications when they become available, visit the Fund's website and register to receive Fund email alerts.
Commonwealth Fund pub. 1657
Vol. 4
Since the 1990s, information and communications technologies—including tele- health—have been at the core of the Veterans Health Administration’s (VHA’s) successful system-level transformation toward providing continuous, coordinated, and comprehensive primary and specialist care services. The VHA’s leadership and culture; underlying health information technology infrastructure; and strong commitment to standardized work processes, policies, and training have all con- tributed to the home telehealth program’s success in meeting the chronic care needs of a population of aging veterans and reducing their use of institutional
care and its associated costs. The home teleheath model also encourages patient activation, self-management, and helps in the early detection of complications.
2 Th e co m m o n w e A lT h Fu n d
Within the VHA, the Office of Telehealth Services (OTS) uses health informatics, disease man- agement, and telehealth technologies to support the remote provision of services and improve access
to timely care for patients in their homes and local communities (Exhibit 1). The OTS offers veterans a program called Care Coordination/Home Telehealth (CCHT) to provide routine noninstitutional care and targeted care management and case management services to veterans with diabetes, congestive heart failure, hypertension, post-traumatic stress disorder (PTSD), chronic obstructive pulmonary disease, and depression. CCHT uses remote monitoring devices in veterans’ homes to communicate health status and to capture and transmit biometric data that are monitored remotely by care coordinators.
In fiscal year 2010, an estimated 300,000 patients received care across all programs within OTS. CCHT, which targets patients at risk for long-term institutional care (approximately two-thirds of the cur- rent CCHT population), currently manages more than
70,000 veteran patients using home telehealth tech- nologies. The program has demonstrated successful outcomes. Through the end of fiscal year 2010, veter- ans reported patient satisfaction levels greater than 85 percent for home telehealth services offered through CCHT. In addition, the program was associated with
a greater than 40 percent reduction in bed days of
care, as compared with pre-enrollment figures, for the
CCHT population receiving home telehealth.1
Organizations outside the VHA can learn from its home telehealth experience. Core principles in suc- cessful implementation include: a recognized respon- sibility for the care and case management of patients across the continuum; a systematic approach to the introduction of a quality performance improvement and management infrastructure; contracting with technol- ogy vendors on a national scale; and implementation that is driven at the local clinical level to ensure that benefits can be derived immediately. This is supported by a tremendous organizational readiness and capacity for change that is embodied in all areas of practice. The ability to directly control budgets for care services is also a strong motivator in making home telehealth pro- grams work. While complementary infrastructure ele- ments at the VHA, including electronic health records (EHRs), help make home telehealth operational at an organizational level, they are not necessarily required for a program to work.
From an organizational perspective, it may be easiest for other integrated delivery networks or government-sponsored systems to draw lessons from the VHA’s experience, particularly where there is a recognized responsibility for the care and case man- agement of patients across the continuum. In terms of care management and patient care coordination needs, the lessons of the VHA may be most applicable to the dual-eligible population.
Telehealth involves the use of information and communications technologies to deliver medical care remotely by connecting multiple users in separate locations. The VHA Office of Telehealth Services uses health informatics, disease management, and telehealth technologies to facilitate access to care and improve health outcomes in three main ways:
of care.
Source: U.S. Department of Veterans Affairs, VHA Office of Telehealth Services, “What Is Telehealth?” (Washington, D.C.: U.S. Department of Veterans Affairs, 2011).
Th e Ve T e r A n s he A lT h Ad m i n i s T r AT i o n : TA k i n g ho m e Te l e h e A lT h se rV i c e s To sc A l e nAT i o n A l ly 3
BACKGROUND
The Veterans Health Administration within the U.S. Department of Veterans Affairs (VA) is regarded as a modern, responsive, efficient, and effective health care organization that many hold up as a model for deliver- ing cost-effective, quality outcomes. While it faces similar financial and clinical challenges as other health care delivery organizations, the VHA is unique in
terms of the health care needs it addresses among the veteran population and in being directly accountable to Congress and financed primarily from public budgets. As one of the nation’s largest integrated health care systems, the VHA’s primary and specialty care ser- vices serve approximately 6 million veterans with an annual budget of more than $50 billion. It is organized around a service network model rather than hospitals. Each of the 21 Veterans Integrated Service Networks (VISNs)—or shared systems of care—operates with accountable clinical leadership responsible for mak-
ing basic budgetary, planning, and operating decisions
(Exhibit 2).
The shift toward continuous, coordinated, and comprehensive primary and specialist care services started in the mid-1990s.2 Observers have attributed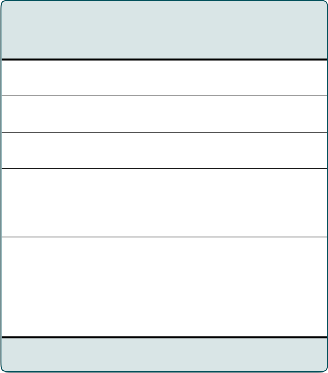
the VHA’s successful transformation from a bottom- to
Projected U.S. veterans population 22,328,000
Female 10%
65 years or older 42.1%
a top-performing health care organization to a combi- nation of factors, including a strategic vision and com- pelling case for system-level transformation; leadership support and shared decision-making authority between officials in the central office and regional managers
and key personnel at the local level; continuous and accountable performance improvement processes tar- geted toward incentivizing the delivery of interdisci- plinary, team-based, patient-centered, quality care ser- vices at a reasonable cost; and a technology architec- ture that has served as the backbone for implementing enterprise-wide EHRs and health information systems and allowing the organization to align its mission with quantifiable strategic goals and performance indica- tors. The potential value to the VA from investments in health information technology is just over $3 billion in cumulative benefits (net of investment costs) through reductions in unnecessary and redundant care, process efficiencies, and improvements in care quality.3
Reducing hospital readmissions has been an important performance improvement goal at the VHA. Higher readmission rates within the VHA have been generally associated with patients who are at
an increased distance from the admitting facility and experience higher comorbidity scores.4 In fiscal year
2009, the VHA reported that the 30-day unadjusted
all-cause readmission rate averaged 12.7 percent (with a range of 0 to 17.7%) across the VHA health care sys- tem. During this period there were 485,774 acute medi- cal/surgical discharges and 81,634 mental health hos- pital discharges reported by the VHA. The unadjusted readmission rate for congestive heart failure was higher than the VHA national average (20.2%) at 12 facilities and significantly lower than the VHA national average at 10 facilities.5 Structural and organizational interven-
White Black Hispanic
Total enrollees
Total unique patients treated
2011 appropriations (actual) Hospitals
Community-based outpatient clinics
Source: National Center for Veterans Analysis and Statistics.
83.0%
11.9%
6.1%
8.57 million
6.17 million
$51.5 billion
152
817
tions using technology, like telehealth, are particularly promising in terms of offering improved access to health care and providing superior quality of care.
Care Coordination/Home Telehealth was developed by the VHA to respond to the rising number of elderly veterans with chronic care needs and reduce their use of institutional care and its associated high costs. Group Health’s Chronic Care Model serves as the conceptual framework for CCHT and has helped
4 Th e co m m o n w e A lT h Fu n d
move toward the goal of making the patient’s home into the preferred place of care where possible and appropriate.6 Promoting patient activation and self- management is fundamental in the CCHT model to prevent unnecessary hospital admissions or emergency department visits. The VHA’s experience indicates that the messaging functionality within home telehealth ser- vices supports this goal through proactively identifying adverse symptoms, knowledge deficits, and negative health-related behaviors. Reduced use of health care resources for CCHT’s patient population is attributed
to patient self-management, disease management, and the use of virtual visits.
HOME TELEHEALTH: TAKING A PROGRAM FROM INITIAL PILOT TO SCALE
Today, the VHA is the largest individual purchaser of home telehealth technology worldwide and it plans
to increase the size of its program considerably. The VHA’s history has made it the health care industry’s test case for how to successfully plan and implement a
program that has been embraced throughout the organi- zation from senior leadership to the patient population. However, the VHA has faced many of the same chal- lenges as other health care organizations in implement- ing technology into care delivery practice. Namely, scaling a process that reproduces the financial and care outcomes from pilots while ensuring sustainability of the clinical, technology, and business processes neces- sary to support home telehealth.
Implementation at the VHA has centered around reengineering existing processes, a strong IT infrastructure, and a commitment to training. The VHA attributes the rapidity and robustness of its CCHT implementation to the systems approach taken to inte- grate the clinical, technology, and business elements
of the program based on its experience with pilot programs. For example, CCHT incorporated existing business processes wherever possible to reduce the program’s overhead costs and increase efficiency. The VHA experience demonstrates that implementation
at scale is possible and can yield substantial returns across both time and geography. Dr. Adam Darkins,
who oversees CCHT, adds that the basic care needs, staffing, and use of technology to coordinate care,
as well as design and operational details will vary to accommodate differences in health care delivery orga- nizational models.
The current program’s origins date back to
the mid-1990s, although the VHA’s involvement with telemedicine dates back to 1977 when it piloted the use of telemedicine in Nebraska. Home telehealth
as discussed in this case study only came to the fore in the mid-1990s, when it was introduced to address patient need. The primary goals were to expand access, provide care as close as possible to the patient’s com- munity, and make the home the preferred place of
care when appropriate. The clinical leadership of the regional VISN in South Florida and the Caribbean, VISN 8, originally conceived the program with the goal of creating a cost-effective mode of avoiding higher-cost institutional care and supporting aging vet- erans in their homes and communities. The initial pilot focused on the 4 percent of the noninstitutionalized veteran population in the network who were driving approximately 40 percent of costs.7
VISN 8 conducted a telehealth pilot from 2000 to 2003 in its integrated system of seven hospitals, 10 multispecialty outpatient clinics, and 28 community- based primary care clinics. With a population of approximately 900 patients, the pilot included moni- toring along with patient self-management and use of relatively simple home telehealth devices. The pilot
was associated with a 40 percent reduction in emer- gency room visits, a 63 percent reduction in hospital admissions, and an 88 percent reduction in nursing home bed days of care, as well as a high (94%) level of patient satisfaction. The pilot formed the basis for
the model that was implemented nationally in the VHA
after 2003.8 The national model also achieved high rates of patient satisfaction and reductions in resource utilization.
When developing the national program, the VHA’s senior leadership was committed to putting into place the necessary infrastructure. Core elements included developing algorithms for selecting patients
Th e Ve T e r A n s he A lT h Ad m i n i s T r AT i o n : TA k i n g ho m e Te l e h e A lT h se rV i c e s To sc A l e nAT i o n A l ly 5
and matching them to the right technology (e.g., video- phones, messaging devices, biometric devices, digital cameras, and telemonitoring devices); establishing a national training center to ensure a competent work- force; awarding national contracts for technology,
based upon meeting strict clinical and technological requirements; and integrating telehealth technologies with the VHA’s electronic medical record.9 Although the growth of the national home telehealth program has been managed largely at a VISN level to meet the needs of the veteran patient population each serves,
the enabling clinical protocols, workforce training, and business processes have been developed at the national level. Today, CCHT programs are available at 140
VHA medical centers. Forty percent of veteran patients receiving care via CCHT live in rural or remote locations.
Resistance from clinicians has been success- fully addressed by placing the emphasis on program outcomes, patient satisfaction, and training. The VHA has established strategic communications initiatives, like an annual telehealth meeting for key staff from around the country. In addition, a number of staff mem- bers who helped start the program are now in senior management within the organization and have effec- tively become champions of the telehealth program. Meanwhile, graduates of the national training program have gone on to serve as advocates for the program. Dr. Darkins describes their role as critical in helping solve programmatic issues at the local level and serving as ambassadors for the program. This has helped informa- tion about the program grow at an organizational level, increasing buy-in and understanding.
CCHT AND THE HOME TELEHEALTH PROGRAM
First introduced into the VHA in 2003, CCHT uses home telehealth and disease management technologies in the care management of chronically ill patients to delay, if not prevent, their being placed into long-term institutional care. Between 2003 and 2007, CCHT patients increased from 2,000 to 31,570.10 Today, the number of patients managed using home telehealth
technologies at the VHA for noninstitutional care, chronic disease management, acute disease manage- ment, and health promotion and disease prevention is almost 70,000. The VHA plans to have 92,000 people enrolled in its telehealth program by the end of 2012.11
The most commonly used technologies in CCHT are messaging and monitoring devices (85%), followed by videotelemonitors (11%) and videophones (4%). Messaging devices ask patients questions to help
assess their health status and disease self-management capabilities. Monitoring devices record vital sign data. Videophones and videotelemonitors facilitate audio– video consultations at home.
The VHA has used home telehealth services for managing chronic conditions at an unprecedented scale compared with other health service organiza- tions. The VHA’s underlying health information infrastructure, coupled with a strong commitment to standardized work process, policies, and training, has contributed to the increase in the program’s capacity to manage an increasing volume of patients. Of patients enrolled in the program between 2003 and 2007, 96 percent were male and 4 percent were female. The
age range was 20 to 101 years, with a mean of 66.5 years and 16.5 percent of patients 85 years and older. About 57 percent lived in urban areas, 37 percent in rural areas, and 2 percent in highly rural areas. About
48 percent of patients were managed for diabetes, 40 percent for hypertension, 25 percent for congestive heart failure, 12 percent for chronic obstructive pul- monary disease, 2 percent for depression and 1 percent for PTSD.12 Almost 67 percent were monitored for one condition, and 33 percent for multiple conditions.
Within CCHT, care is actively managed by care coordinators who are health care professionals, usually nurses or social workers, but who also include dieticians, occupational therapists, physicians, and pharmacists. An individual care coordinator handles
a panel of 100 to 150 general medical patients or
90 patients with mental health-related conditions. Care coordination is managed in association with the patient’s clinician, and referrals to additional care ser- vices can be made by the care coordinator (subject to
6 Th e co m m o n w e A lT h Fu n d
appropriate delegation and scope of practice) without the patient having to be automatically seen by a pri- mary care physician.
Ensuring the VHA has a competent telehealth workforce has been a critical component of its strategy to expand services nationwide. Standard professional training does not include telehealth. To remedy this situation, the VHA has established a dedicated national CCHT training center. Formal telehealth certification does not exist, but the VHA ensures regular competency assessments and requires that staff are trained as part of its internal reviews of telehealth programs. Care coor- dinators undergo a three-to-five-week intensive train- ing course in the requisite skills and competencies. The center has trained over 5,000 staff members, to date.
Eligible patients are offered the choice to receive CCHT-based care or other noninstitutional care services. Among those offered home telehealth, only
10 percent prefer to use the more traditional in-person encounters. When a patient is enrolled, the care coor- dinator selects the appropriate home health technol- ogy using an algorithm based on a patient’s needs, the complexity of the disease or condition, and the indi- vidual’s ability to use technology. The algorithm helps determine which CCHT device (videophone, messag- ing device, biometric device, digital camera, or tele- monitoring device) is most suitable and cost-effective for each patient’s use. Upon device selection, the care
coordinator gives the patient and caregiver the required training.13
On an ongoing basis, the coordinator reviews telehealth monitoring data and provides active care
or case management. Each patient is classified on the basis of his or her risk level, which is assessed daily according to preset thresholds, with alerts if any signif- icant changes arise in the patient’s symptoms or behav- ior that require intervention and management. When alerts occur, care coordinators intervene as necessary. For instance, a coordinator may call a patient to verify
a potential exacerbation of their condition to prevent an emergency room visit or hospitalization.
Care coordinators coordinate patients’ care even when they receive care services outside the VHA
system. The VHA also provides patients with the abil- ity to authorize sharing of electronic patient record data, such as prescriptions or lab results, through the
“Blue Button” application. Blue Button is a convenient and secure method for patients to retrieve information in plain text via the Internet. In addition to the 6 mil- lion veterans who receive care through the VHA, the VHA plans to also make the Blue Button application available to the 17 million veterans who receive care at non-VHA health providers and hospitals.14
EVIDENCE OF OUTCOMES IN HOME TELEHEALTH
The VHA has found that an enterprise-wide home telehealth system is an appropriate and cost-effective means of managing chronic care patients in both urban and rural settings. Studies that compared data from
the year before entering the program and six months postenrollment show a 25 percent reduction in bed days of care, a 20 percent reduction in number of admissions, and a mean satisfaction score rating of 86 percent. Decreases in health resource utilization were largest in highly rural (50.1%) and urban (29.2%) areas, for mental health-related conditions, and for patients with multiple conditions. Patients’ acceptance of CCHT was high, with only 10 percent declining services. The cost for CCHT ($1,600 per patient per
year) compared favorably with the direct cost of VHA’s home-based primary care services ($13,121 per patient per year) and market nursing home care rates (an aver- age of $77,745 per patient per year).
Exhibit 3 summarizes the reduction in health care resource utilization (defined as hospital days
of stay) by the condition monitored and for patients monitored for single or multiple diagnoses. There is wide variation across conditions. Although the reasons accounting for such variation are not exactly clear,
the most likely explanation is a reflection of the case mix in that disproportionate numbers of patients are involved for specific conditions as well as the fact that certain conditions affect patients more severely than others.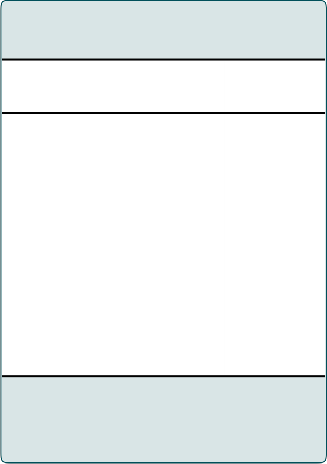
Th e Ve T e r A n s he A lT h Ad m i n i s T r AT i o n : TA k i n g ho m e Te l e h e A lT h se rV i c e s To sc A l e nAT i o n A l ly 7
to expand access to care services and make the home the preferred place of care. The decision to imple-
ment telehealth received strong support from the VHA
leadership, and a telehealth pilot involving the remote
monitoring and patient self-management of nearly 900 patients was launched in 2000. The results of the pilot,
Diabetes 8,954 20.4
Hypertension 7,447 30.3
which demonstrated reductions in hospital admissions and bed days of care as well as high levels of patient
Congestive heart failure
Chronic obstructive pulmonary disease
Post-traumatic stress
4,089 25.9
1,963 20.7
satisfaction, formed the basis for the model that has become the national standard in the VHA since 2003.
Although initial evidence for an innovation is necessary, it is often not sufficient for widespread dif-
disorder 129 45.1
Depression 337 56.4
Other mental health 653 40.9
Single condition 10,885 24.8
Multiple conditions 6,140 26.0
Source: A. Darkins, P. Ryan, R. Kobb et al., “Care Coordination/Home Telehealth: The Systematic Implementation of Health Informatics, Home Telehealth, and Disease Management to Support the Care of Veteran Patients with Chronic Conditions,” Telemedicine and e-Health, Dec. 2008
14(10): 1118–26.
Leaders of other health care organizations
have been dismissive of the applicability of the VHA’s results, noting that the VHA is both payer and pro- vider and therefore has completely aligned incentives and underlying systems for aggressive management
of chronic diseases. However, other programs—some in highly fragmented environments—have been able to achieve similar results to those of the VHA. For instance, the Health Buddy Project, a Medicare tele- health demonstration project, was able to enroll more
than 700 patients in two areas of the Pacific Northwest. The program’s first phase, from 2006 to 2009, showed
a 240 percent return on investment for Medicare.15
KEY SUCCESS FACTORS IN TAKING HOME TELEHEALTH FROM PILOT TO SCALE
The VHA first considered a role for telehealth in noninstitutionalized care in the mid-1990s. Rather than technology being the driver, the impetus for introducing telehealth was the need to address the care demands of chronically ill, aging veterans and
fusion. Ongoing monitoring of the clinical outcomes has demonstrated repeatedly high levels of patient satisfaction and reduced resource utilization and has supported the continued growth of telehealth within the VHA, validated the positive benefits, and strengthened the program’s ability to spread home telehealth ser- vices more broadly throughout the organization.
The VHA’s experience with home telehealth programs highlights the potential of alternatives to traditional care models to drive substantial benefits. The experience also demonstrates that implementation at scale is possible and can yield substantial returns across both time and geography. Successful implemen- tation was centered around reengineering of existing processes coupled with a strong IT infrastructure and a commitment to training.
The following are key factors that have led to the VHA’s ability to successfully pilot and implement home telehealth at scale.
Systematic evidence of targeted outcomes. The pilot program validated the evidence initially found in the literature of small-scale interventions suc- cessfully using home telehealth with chronic disease patients to support independent living and reduce hospital admissions. The program has continued to
demonstrate systematic evidence of targeted outcomes: reductions in bed days of care and hospital admissions, as well as high levels of patient satisfaction, all with- out diminishing the health status of participants. Such evidence has been important in expanding the scale of the program. As it has grown, the evidence has made a
8 Th e co m m o n w e A lT h Fu n d
strong clinical and business case that facilitates buy-in from clinicians and managers. The VHA has found that disseminating its findings broadly throughout the sys- tem, through an annual meeting for key staff members and a quarterly newsletter, for instance, reinforces the continuous cycle of learning within the organization.
Standardization of core program elements. From the outset, the VHA tried to systemize clinical, technological, and business processes. A core principle of this standardized approach has been national poli- cies and operational procedures that ensure the care
a veteran receives is consistent throughout the VHA system. In addition, care coordinators monitor core biometric data and changes in patients’ health status, provide support to patients through education and self- management, and intervene to prevent patients’ clinical deterioration and avoidable hospital admissions.
Technology-enabled tools and resources. The electronic patient record is a critical tool that enables just-in-time decisions that support patient care, particularly in chronic care management. The VHA’s electronic health information system, VistA, has been instrumental in providing a technical health informa- tion infrastructure that supports systemwide imple- mentation of the home telehealth program. Another important technological tool is the algorithm the VHA uses to match patients to appropriate technologies. The home telehealth devices have been chosen for their simple user interface design and ease-of-use to ensure they can be implemented systematically among a very large number of patients and perform reliably.
Staff training and development. The OTS has established national training centers dedicated to each of its three telehealth service areas with the capac- ity to facilitate remote training and to train hundreds of staff members each year. A robust training program has helped contribute to overcoming the initial resistance that clinicians have had to the telehealth approach. The training program for CCHT has also created a cohort
of graduates who serve as ambassadors for the program and who can help solve programmatic issues at the
local level.
FUTURE OPPORTUNITIES AND CHALLENGES IN MAINTAINING HOME TELEHEALTH AT SCALE
While the VHA has become known for its focus on infor- mation technology, pioneering research, high quality of care, and remote health services, the organization con- tinues to face challenges in translating theory and pilots into mainstream services and in ensuring the sustainabil- ity of the clinical, technology, and business processes necessary to support home telehealth. Looking forward, the VHA faces a number of related goal-driven challenges.
Realizing greater economies of scale. CCHT has cited reduced health care resource use among the targeted high-utilization patients. This impact provides strong economic justification for home telehealth to
be an integral component of standard noninstitutional- ized care services for chronically ill veterans at risk
for long-term institutional care. Because of the lower marginal cost of adding services to the existing infra- structure, the VHA is intent on expanding its CCHT program to provide chronic care management, acute care management, and health promotion and disease management for other patients in areas such as weight management, dementia care, and palliative care. In April 2011, the VHA awarded six national contracts for home telehealth devices and services worth $1.38 bil- lion over five years.
Advancing integrated models of care. Many veterans rely on providers other than the VHA for services, which complicates efforts to coordinate their care. This is particularly challenging as the VHA uses a primary care model that adheres to clinical guide-
lines and sharing of information among providers. The advent of a patient-centered medical home model on a national scale is leading the VHA to think about how care coordination for home telehealth can evolve and contribute to successful care management that ensures patients receive the right care in the right place at the right time and that patient engagement and adherence are enhanced. This issue will become increasingly important as more care takes place in the home and community, with informal caregivers playing a central
Th e Ve T e r A n s he A lT h Ad m i n i s T r AT i o n : TA k i n g ho m e Te l e h e A lT h se rV i c e s To sc A l e nAT i o n A l ly 9
role and with individuals encouraged to take on greater responsibility for their own health management.
Adapting to continuous technological change. The VHA is looking at new and emerging technologies, such a social media and mobile devices, to aid in delivering care remotely. There are profes- sional, ethical, technological, regulatory, legal, organi- zational, and risk management issues that apply to how these new technologies will be implemented, and the VHA is addressing these. The VHA also has launched numerous technology initiatives to transform itself
into a 21st century organization that is people-centric, results-driven, and forward-looking. Through a new program called the Innovation Initiative, the VA has committed to being on the cutting edge of health care delivery and laying the foundation for safe, secure, and authentic health record interoperability. By tapping into the talent and expertise of individuals both inside and outside the organization, the VA seeks to identify new, innovative solutions that will increase veterans’ access to VHA services, improve the quality of services, enhance the performance of VA operations, and reduce or control the cost of delivering those services that vet- erans and their families receive.
CONCLUSION
Because the Department of Veterans Affairs operates a large integrated delivery system financed primarily by public money, drawing lessons from the VHA’s experi- ence may be easiest for other integrated delivery net- works or government-sponsored systems. The lessons of the VHA may be most applicable to the population that most resemble veterans targeted for CCHT: dual- eligibles who tend to receive care services through a
fee-for-service model. Telehealth-based care coordina- tion and management will have an impact on the qual- ity of life and care, as well as costs associated with this population. But implementation of programs will likely need to be accompanied by the ability to reproduce the VHA’s underlying systemness to comprehensively sup- port the patient population.
Organizations can learn from the VHA’s home telehealth experience on a number of levels. In particu- lar, by using the core principles that have guided the implementation at scale: a recognized responsibility
for the care and case management of patients across the continuum; a systematic approach to the introduc- tion of a quality performance improvement and man- agement infrastructure; contracting with technology vendors on a national scale; and implementation that is driven at the local clinical level. In addition, the VHA has a tremendous capacity for change that is instilled in the organizational culture from the national leadership
and is embodied in all areas of practice.
ho w Th i s cA s e sT u d y wA s co n d u c T e d

This case study was developed through interviews with staff from the VHA’s Care Coordination/Home Telehealth (CCHT) program and an examination of peer-reviewed journals, articles, and websites of the Department of Veterans Affairs. In particular, the authors would like to acknowledge Dr. Adam Darkins, who oversees the VHA’s CCHT, and his staff.
The other organizations profiled in our Case Studies in Telehealth Adoption series are Partners HealthCare’s Connected Cardiac Care Program and Centura Health’s Centura Health at Home program. To read them, along with a synthesis of findings from all three case studies, visit our website at http://www.commonwealthfund.org/ Publications/Case-Studies/2013/Jan/Telehealth-Synthesis.aspx.
10 Th e co m m o n w e A lT h Fu n d
no T e s
1 A. Darkins, “Telehealth Continues to Make Its
Mark,” VHA Telehealth Quarterly, Oct. 2010
10(1):2.
2 P. Longman, Best Care Anywhere. Why VA Health Care Is Better Than Yours (Sausalito, Calif.: Poli- Point Press, 2007).
3 C. Byrne, L. M. Mercincavage, E. C. Pan et al., “The Value from Investments in Health Information Technology at the U.S. Department of Veterans Af- fairs,” Health Affairs, April 2010 29(4):629–38.
4 S. M. Kehle, N. Greer, I. Rutks et al., Interventions to Improve Veterans Access to Care: A Systematic Review of the Evidence, VA-ESP Project #09–009
2011 (Washington, D.C.: Veterans Health Adminis- tration, Health Services Research and Development Service, Jan. 2011).
5 Veterans Health Administration, 2010 VHA Facil- ity Quality and Safety Report (Washington, D.C: . Veterans Health Administration, Office of Quality and Safety, Oct. 2010).
6 E. H. Wagner, “Chronic Disease Management: What Will It Take to Improve Care for Chronic Illness?” Effective Clinical Practice, Aug./Sept. 1998 1(1):2–4.
7 R. Kobb, N. Hoffman, R. Lodge et al., “Enhancing Elder Chronic Care Through Technology and Care Coordination: Report from a Pilot,” Telemedicine Journal and e-Health, June 2003 9(2):189–95.
8 Ibid.
9 D. Lindeman, “Interview: Lessons from a Leader
in Telehealth Diffusion: A Conversation with Adam Darkins of the Veterans Health Administration,” Ageing International, Oct. 2, 2010 36(1):146–54.
10 A. Darkins, P. Ryan, R. Kobb et al., “Care Coordi- nation/Home Telehealth: The Systematic Implemen- tation of Health Informatics, Home Telehealth, and Disease Management to Support the Care of Veteran Patients with Chronic Conditions,” Telemedicine Journal and e-Health, Dec. 2008 14(10):1118–26.
11 M. Freudenheim, “Wired Up at Home to Monitor Illnesses,” New York Times, Nov. 22, 2010, Health section, http://www.nytimes.com/2010/11/23/ health/23monitor.html.
12 Numbers reflect multiple comorbidities.
13 P. Ryan, R. Kobb, and P. Hilse, “Making the Right Connection: Matching Patients to Technology,” Telemedicine Journal and e-Health, 2003 9(1):1–8.
14 For more information, see http://bluebuttondata.org.
15 L. C. Baker, S. J. Johnson, D. Macaulay et al., “In- tegrated Telehealth and Care Management Program for Medicare Beneficiaries with Chronic Disease Linked to Savings,” Health Affairs, Sept. 2011
30(9):1689–97.
Th e Ve T e r A n s he A lT h Ad m i n i s T r AT i o n : TA k i n g ho m e Te l e h e A lT h se rV i c e s To sc A l e nAT i o n A l ly 11
AB o u T T h e Au T h o r
Editorial support was provided by Deborah Lorber.
These case studies were based on publicly available information and self-reported data provided by the case study institutions. The
Commonwealth Fund is not an accreditor of health care organizations or systems, and the inclusion of an institution in the Fund's case study series is not an endorsement by the Fund for receipt of health care from the institution.

